What Is Asthma?
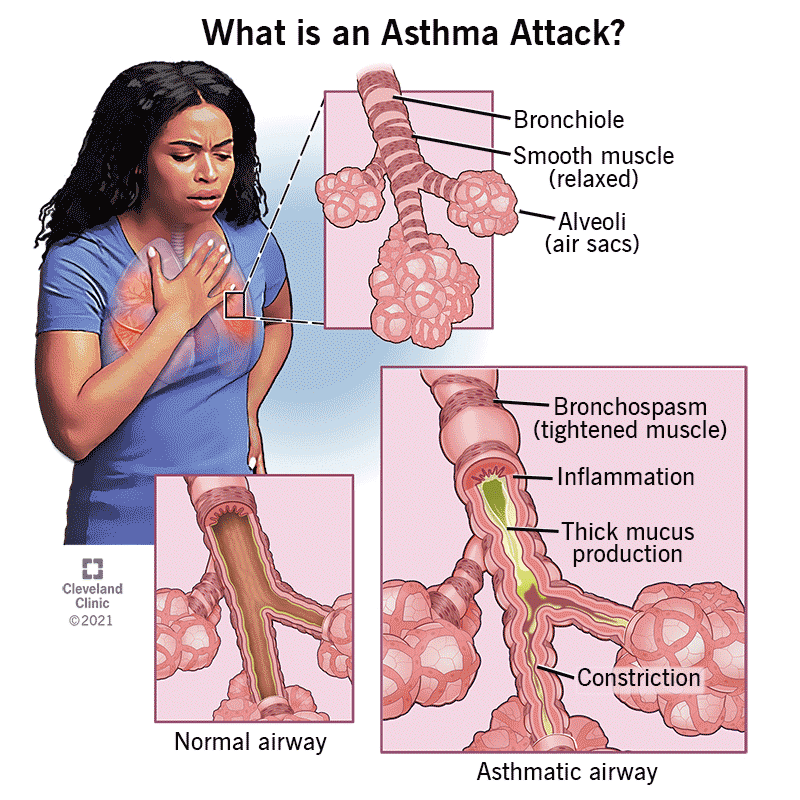
Asthma is a chronic inflammatory disease of the airways that causes recurring episodes of wheezing, breathlessness, chest tightness, and coughing — particularly at night or in the early morning. During an asthma episode, the airways become inflamed and narrowed, and mucus production increases, making it difficult to breathe. Between episodes, most people with well-controlled asthma feel normal. However, untreated or poorly controlled asthma can significantly limit daily activities and, in severe cases, lead to life-threatening exacerbations.
Asthma affects approximately 25 million Americans and is one of the most common chronic respiratory conditions seen by pulmonologists. Although it cannot be cured, asthma can be effectively managed in the vast majority of patients. When symptoms remain difficult to control despite standard therapy, further evaluation by a pulmonologist is essential to identify underlying causes, rule out mimicking conditions, and determine whether advanced treatments such as biologic medications are appropriate. Request an evaluation →
Asthma Care at PulmoCrit
Spirometry & bronchodilator testing — objective confirmation of airflow obstruction and reversibility
FeNO testing — fractional exhaled nitric oxide to measure eosinophilic airway inflammation
Severe & difficult-to-treat asthma — specialist workup for patients failing standard inhaler therapy
Biologic therapy — evaluation and initiation of dupilumab, mepolizumab, benralizumab, and other targeted agents
Allergy & trigger evaluation — identifying occupational, environmental, and seasonal triggers
Cough-variant asthma — diagnosis and treatment of asthma presenting primarily as chronic cough
Available at Granada Hills, Encino, and Thousand Oaks. Request an appointment →
What causes asthma and who is at risk?
Asthma results from a combination of genetic and environmental factors. A family history of asthma or other allergic conditions — such as eczema or hay fever — increases the risk. Common environmental triggers include allergens (dust mites, pet dander, mold, pollen), respiratory infections, exercise, cold air, tobacco smoke, air pollution, and occupational exposures such as chemical fumes or dust. In some individuals, aspirin or NSAIDs can trigger asthma, a pattern known as aspirin-exacerbated respiratory disease (AERD). Asthma can develop at any age, though it most commonly begins in childhood. Adults who develop asthma for the first time often have non-allergic forms of the disease, which can be more difficult to treat.
Types of asthma
Not all asthma is the same. Understanding the underlying type helps guide treatment:
-
Allergic (atopic) asthma — the most common type, triggered by allergens; often associated with eczema and hay fever. Responds well to inhaled corticosteroids and, in severe cases, biologics targeting IgE (omalizumab) or IL-4/IL-13 (dupilumab).
-
Eosinophilic asthma — a type of severe asthma driven by eosinophil inflammation. Identified through blood eosinophil counts, FeNO testing, and sputum analysis. Responds dramatically to anti-IL-5 biologics (mepolizumab, benralizumab) and anti-IL-4/13 therapy (dupilumab).
-
Non-allergic (non-atopic) asthma — triggered by cold air, exercise, stress, or respiratory infections rather than allergens. More common in adults. Often requires higher-dose inhaled corticosteroids and careful evaluation for other contributing factors.
-
Exercise-induced bronchoconstriction (EIB) — airway narrowing triggered by physical activity. Can occur with or without underlying asthma. Diagnosed with exercise challenge testing and treated with pre-exercise bronchodilators.
-
Occupational asthma — caused or worsened by workplace exposures to sensitizers (isocyanates, latex, flour) or irritants. Accurate diagnosis requires detailed occupational history and sometimes serial peak flow monitoring at work and away.
-
Cough-variant asthma — asthma presenting primarily as a persistent dry cough without typical wheezing or breathlessness. Often missed or misattributed to other causes. Diagnosed with spirometry, bronchodilator response, and/or methacholine challenge.
What are the symptoms of asthma?
Asthma symptoms vary from person to person and may change over time. Common symptoms include:
-
Wheezing — a high-pitched whistling sound when breathing, especially on exhaling
-
Shortness of breath, particularly with exertion or exposure to triggers
-
Chest tightness or pressure
-
Persistent cough, especially at night, in the early morning, or after exercise
-
Waking at night due to coughing or breathing difficulty
-
Symptoms that flare with colds, respiratory infections, or allergen exposure
How is asthma diagnosed?
Asthma cannot be diagnosed by symptoms alone — objective testing is essential. The cornerstone of diagnosis is spirometry, which measures airflow through the lungs before and after a bronchodilator (rescue inhaler). Reversible airflow obstruction — defined as a significant improvement in FEV₁ after bronchodilator administration — is characteristic of asthma. In patients with normal spirometry but suspected asthma, a methacholine challenge test can be used to assess airway hyperresponsiveness. Additional testing may include:
-
FeNO (fractional exhaled nitric oxide) — a non-invasive breath test measuring eosinophilic airway inflammation; elevated levels support an allergic or eosinophilic asthma diagnosis and predict response to inhaled corticosteroids and biologics
-
Blood eosinophil count — a simple blood test that helps characterize asthma type and guide biologic selection
-
Allergy testing — skin prick tests or specific IgE blood tests to identify allergic triggers
-
Chest imaging — a chest X-ray or CT scan to exclude other conditions that can mimic asthma
-
Peak flow monitoring — daily measurements of maximum airflow speed; variability in peak flow is a diagnostic criterion for asthma and helps monitor control over time
How is asthma treated?
Asthma treatment is step-based — the intensity of therapy is matched to symptom severity and frequency. The primary goals are to achieve and maintain symptom control, prevent exacerbations, and preserve normal lung function with the minimum effective medication burden.
-
Short-acting bronchodilators (SABAs) — albuterol and similar rescue inhalers relax airway muscles quickly during symptoms. Frequent use signals inadequate control and the need for step-up therapy.
-
Inhaled corticosteroids (ICS) — the most effective long-term controller medications for most asthma patients. They reduce airway inflammation and decrease the risk of exacerbations. Consistent daily use is essential; they do not provide immediate relief.
-
ICS/LABA combinations — adding a long-acting bronchodilator (LABA) to an inhaled corticosteroid improves control in patients not adequately managed on ICS alone. Common examples include fluticasone/salmeterol and budesonide/formoterol.
-
Leukotriene receptor antagonists (LTRAs) — montelukast can be used as an add-on or alternative controller, particularly useful in patients with allergic asthma or exercise-induced symptoms.
-
Biologic medications — for patients with severe asthma not controlled by high-dose ICS/LABA therapy, biologics targeting specific inflammatory pathways represent a major advance. Options include omalizumab (anti-IgE), mepolizumab and benralizumab (anti-IL-5), dupilumab (anti-IL-4/13), and tezepelumab (anti-TSLP). The right biologic depends on the patient's asthma phenotype, eosinophil count, FeNO level, and IgE level.
When to see a pulmonologist for asthma
While many patients with mild asthma are managed by their primary care physician, a referral to a pulmonologist is appropriate when symptoms remain uncontrolled despite appropriate treatment, when the diagnosis is uncertain, when frequent exacerbations occur, when oral corticosteroids are needed repeatedly, or when biologic therapy is being considered. Pulmonologists also have access to advanced diagnostic testing — including bronchial challenge testing, FeNO, and comprehensive pulmonary function testing — that is not typically available in primary care settings.